The number of ambulance transports by ambulance continues to increase year by year, and in 2019, about 6 million people were transported nationwide. The transportation of elderly people accounts for 60%, and along with this, problems such as "whether or not to respect the will of the person or family" regarding first aid are increasing, and the emergency site is busy dealing with it.

This summer, the temperature has been high nationwide since the beginning of August, and the number of people being transported by emergency on suspicion of heat stroke has increased rapidly. According to the Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, 35,317 people were transported nationwide from June 1st to August 16th, 2020 due to heat stroke. In the week from August 10th to 16th, about one-third of them, 12,804 people, were transported by emergency. It doubled from 6,664 in the previous week (August 3-9), and greatly exceeded 7,639 in the same period of the previous year. By age group, "elderly people" aged 65 and over accounted for 61.8%, followed by "adults" aged 18 and under 65 years old at 31.1%.
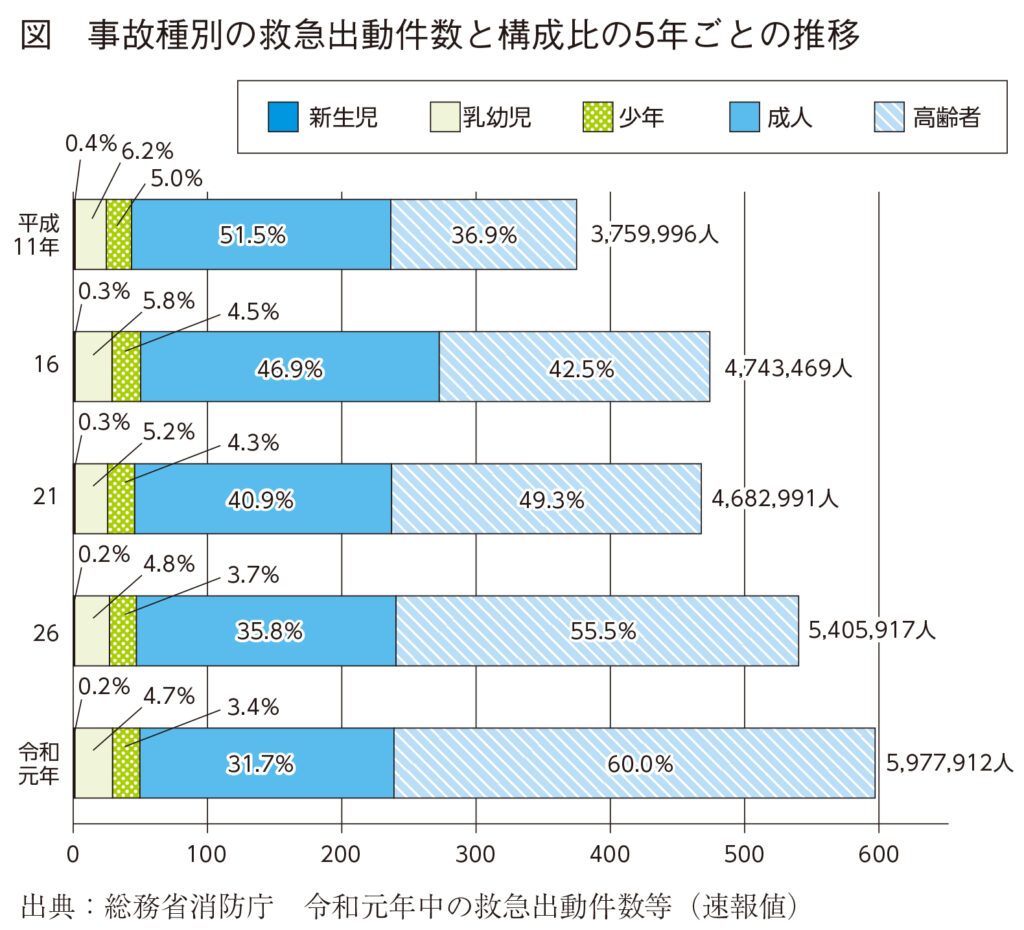
In recent years, the number of cases of transporting elderly people has continued to increase in emergency transportation. The number of people transported by emergency in 2019 was 5,977,912, a record high, and has increased about 1.6 times in the 20 years since 1999 (Fig.). In the last 20 years, the number and ratio of emergency transport for the elderly has continued to increase 2.6 times from that of 1999, and in 2019, 60.0% of all transporters will be elderly.
The increase in emergency transport and the increase in elderly transporters are the result of reflecting the aging of the population. In fact, if the percentage of accident types in which ambulances are dispatched is limited to sudden illnesses, it accounted for 56.3% of the total in 1999, but increased to 65.3% in 2019.
The increase in sudden illness was due to the sudden illness at homes and facilities for the elderly, and the increase in the number of elderly people calling for ambulances. ..
One of them is dealing with people who do not want CPR. The number of cases of cardiopulmonary arrest is increasing year by year, of which 85% are over 60 years old and half are over 80 years old. Since there are many elderly people, there are an increasing number of cases in which family members request that CPR be discontinued, saying that "the person does not want CPR" at the emergency site. In a time-consuming situation, it is difficult for the ambulance crew to decide whether to carry out emergency services while performing resuscitation measures to save lives, or to give priority to the family's opinion that it is the person's intention. ..
According to the 2013 Health and Labor Sciences Research "Questionnaire Survey Results on the Start and Stop of Cardiopulmonary Resuscitation in Emergency Services," 17% of emergency personnel are in a state of cardiopulmonary arrest in writing such as living will. I had experienced cases of not wishing for CPR. On the other hand, the response of the ambulance crew to those who have stated that CPR is not performed (DNAR = Do Not Attempt Resuscitation) differs depending on each fire department, and in the survey conducted by the Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications in 2018, it was decided to use DNAR. 54.4% of the fire departments did not set a response policy.
For this reason, in order to respect the wishes and intentions of the person at the end of life as much as possible, academic societies such as the Ministry of Health, Labor and Welfare, the Japanese Society of Clinical Ethics, and the Japanese Society of Intensive Care, and related organizations have established guidelines for end-of-life care including DNAR. I'm making a suggestion. However, these guidelines are limited to inpatients at medical institutions who can provide life-saving medical care in the event of a sudden change or can give DNAR directives by doctors. Since most elderly people who call ambulances due to sudden illness are at home or in facilities for the elderly, life-saving medical care cannot be performed immediately, and it is still undecided how emergency personnel should handle DNAR directives by doctors and confirm their DNAR intentions. There are no guidelines.
Under these circumstances, the Tokyo Fire Department has announced a policy to introduce DNAR according to the instructions of family doctors from December 2019. Adults who have had an "Life Conference (ACP)" with their families and doctors, are in cardiopulmonary arrest, are in the final stages of their lives, such as the end of malignant tumors, and do not want to perform CPR. Conditions such as having "intention" are required. With this policy, even if a family member calls an ambulance in a hurry due to a sudden change in the patient (cardiopulmonary arrest), the ambulance crew will first contact the family doctor and the family doctor will confirm the death. Is expected to increase in cases where is respected.
Another problem with emergency transportation for the elderly is the "improper use" of ambulances. For example, according to the Tokyo Fire Department, the reason for the actual request for an ambulance for the elderly was "I am planning to be hospitalized, but I called an ambulance because it costs a taxi if I go by myself." I couldn't sleep, so I called an ambulance because I wanted someone to talk to me. "
Improper use of ambulances will result in a shortage of ambulances and will increase the time required for ambulance transport. In fact, the average time required for an ambulance to arrive at the site was 7.7 minutes in 2009, but in 2019 it was extended to 8.7 minutes by 1 minute, and the average time from the arrival of the ambulance crew to hospitalization was also increased. In 2009, it was 35 minutes, but in 2019 it was 39.5 minutes, an increase of 4.5 minutes. Recently, in addition to the response to COVID-19, the problem of difficulty in accepting ambulance patients due to lack of beds and staff is increasing due to the increase in improper use of ambulances.
According to the Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, in the 10 years from 2009 to 2019, the number of patients who were transported by emergency but were diagnosed as mild was about 50% of the total number of patients who were transported by emergency, and the ratio did not increase or decrease much. However, the number of elderly patients diagnosed with mild illness increased by 15 points from 34.1% to 49.0%. In the past, it was thought that among the patients transported by ambulance, those who could return home only by outpatient treatment = mildly ill = inappropriate users, but the number of mildly ill patients increased only because of improper use. It is also possible that the number of people who have been able to deal with injuries and illnesses that were previously hospitalized, but have been able to respond sufficiently to outpatients and return home, has increased due to advances in diagnosis and treatment techniques.
However, he points out that "it is necessary to carefully consider and respond to whether or not to return the patient immediately even if he / she is able to walk" is a professor at the International University of Health and Welfare School of Medicine (emergency medical care at the same university hospital). It is Mr. Takashi Shiga of the department). An actual case was a woman in her 70s who was transported by emergency. The main complaint is weakness. He had no headache, chest pain, or fever, and had mild hyponatremia and dehydration, so when he started the infusion, he said, "I'm fine now, so I want to remove the infusion and go home." He said that he was living alone, 5km to his home, and 500 yen for his wallet, so when he first contacted the Regional Comprehensive Support Center, he received a reply from a well-known inhabitant and left it to him. "Even if you can go home, there are many elderly people who need the support of someone in their daily lives. At the emergency site, it is necessary to take such situations into consideration," says Shiga. Detailed responsiveness with limited resources is also one of the requirements for emergency medical care.
Changes in the number of emergency dispatches by accident type and composition ratio every 5 years
Source: Ministry of Internal Affairs and Communications Fire and Disaster Management Agency Number of emergency dispatches during the first year of Reiwa (preliminary figures)
Ambulances have been improved over time to ensure safe transport of patients and ease of movement for rescuers. In the 1970s, the number of traffic accidents increased, and ambulances were equipped with various devices to provide first aid such as hemostasis and oxygen inhalation until the patient was taken to the hospital.
Nowadays, "high standard ambulances" are becoming the standard. Development of high-standard ambulances has progressed before and after the introduction of the paramedic system in 1992. A car with a high ceiling was introduced to make it easier to move inside the car, the car shook less, and a sleeper (stretcher) was also installed. Various equipment necessary for lifesaving is installed in the car. In addition to medical equipment such as airway management sets and delivery sets required for treatment, PPE, patient monitoring devices (electrocardiogram, pulse wave, blood pressure, blood oxygen saturation), automatic in vitro defibrillators, respirators, etc. Is also installed. Advances in these facilities and equipment are expected to expand the life-saving measures that can be performed on-site or in the car under the instructions and advice of doctors, and improve the life-saving rate of patients.

 Medical equipment in an ambulance
Medical equipment in an ambulance
The challenge of home medical care that "supports daily life" - A "triple win" for patients, medical institutions, and the government will ensure the future of an aging society...

Supporting the career advancement of female doctors Introduce career counseling to increase the number of female doctors aiming to become specialists...

The new value of medical care is to improve the happiness of patients and medical professionals by providing medical services that emphasize "emotional value"

The introduction of Japan's first command center has changed the way nurses work and increased hospital bed occupancy rates

Informed consent in the medical field as seen through court cases (Part 2)